Laparoscopic Gastric Bypass
Summary:
- Experienced, senior team providing a multidisciplinary approach to surgery.
- Price: $10,000-13,000 for patients with Private Health Insurance covering weight loss surgery
Gastric Bypass Surgery
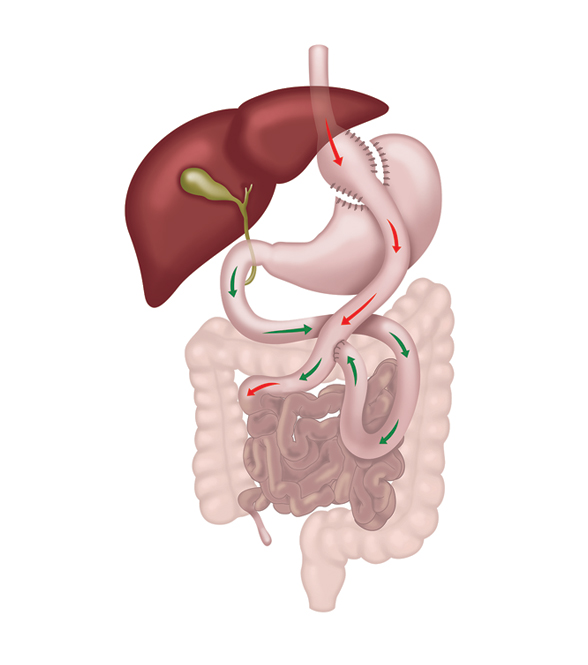
Laparoscopic (keyhole) gastric bypass is a well established obesity surgery which creates a smaller stomach and bypasses part of the small intestine, reducing the absorption of food. At LapSurgery we have been performing this procedure since 2009. It is particularly effective for patients with Type 2 diabetes.
There are several slightly different ways of performing a gastric bypass, at LapSurgery Australia we perform the most commonly used version referred to as a Roux-en-Y gastric bypass. Whilst it is a more complex operation than the sleeve gastrectomy or the gastric band, it can be performed with keyhole surgery.
Gastric bypass, stomach bypass, Roux-en-Y gastric bypass and RYGB all describe this operation. Many surgeons regard it as the gold standard obesity operation, and it is performed as keyhole surgery by our Melbourne bariatric surgeons, with two bariatric trained surgeons at every operation.
The team at LAPSurgery Australia are recognised for their exceptional and major contribution to the Government sponsored Bariatric Safety Registry (BSR). The BSR tracks surgical complications and provides an unbiased safety record for weight loss surgery.
Video Hub
We've created a series of videos to explain details about the weight loss surgery process.
From Appointment to Assessment
1minMarilyn's Story
2minAre you a candidate?
Use our BMI calculator to check your eligibility and get a price estimate.
Related Procedures
Sleeve Gastrectomy
Our most common procedure, reducing stomach size without rerouting the bowel.
Learn moreOne Anastomosis Gastric Bypass
A technically simpler bypass with one join instead of two.
Learn moreSADI Surgery
A newer procedure combining sleeve gastrectomy with intestinal bypass for maximum effect.
Learn moreYour Next Steps
Ready to take the next step? Here is how to get started.
Frequently Asked Questions
Common questions about gastric bypass surgery
Generally a BMI of 35 or above, or 30 or above with a weight related health condition such as type 2 diabetes, sleep apnoea, high cholesterol, gout or liver disease. Lower thresholds apply for people of Asian descent. Our BMI calculator gives you an immediate indication.
Studies comparing the two over five year time frames show very similar weight loss. However, patients with type 2 diabetes or gastric reflux generally have better results with the bypass. At your consultation we present the facts for your situation and you make the decision.
Patients commonly lose 60 to 70 per cent of their excess weight over 18 to 24 months. Individual results vary, and long term success depends on the lifestyle changes our multidisciplinary team supports you through.
Diabetes control typically improves within days of the operation, before significant weight is lost, and many patients achieve long term remission. Outcomes depend on how long you have had diabetes and your individual circumstances, which your surgeon and our Specialist Physician will discuss with you.
From $10,000 to $13,000 for patients with private health insurance covering weight loss surgery, including your surgical team, Specialist Physician, psychologist, dietitian and exercise professional consultations and comprehensive after care. A full written quote is provided after your consultation.
You progress from fluids to pureed foods to soft foods over approximately four to six weeks, then settle into small portions of most food types. Very high fat or high sugar foods can trigger dumping syndrome and are best avoided. Daily multivitamins are essential for life.
Dumping syndrome is a possible side effect of gastric bypass, usually triggered by high fat or high sugar foods, causing symptoms such as nausea, cold sweats, dizziness or diarrhoea. It is most common in the first two to three months, settles quickly, and a visit to our dietitian usually gets things back to normal.
Have more questions? We're here to help.
Contact us for more informationArrange a Consultation
Ready to start your journey? Contact us today — we can help you get a referral and schedule your consultation.
Address
Gladstone Road Consulting Suites 327 Gladstone Road Dandenong North, VIC 3175
Phone
(03) 9760 2777Office Hours
Monday – Friday: 9:00 AM – 5:00 PM Saturday – Sunday: Closed